Retinopathy of Prematurity (ROP)
Introduction and History
Retinopathy of prematurity (ROP), often called “ROP,” is an eye disease that can affect babies born too early (prematurely). It happens because the blood vessels in the retina haven’t finished growing when the baby is born. In ROP, these blood vessels grow abnormally and can lead to serious vision problems, including blindness, if left untreated.
The condition was first described in medical literature by Dr. Theodore Terry in 1942, who called it “retrolental fibroplasia” [1]. In the 1940s and 1950s, ROP caused an “epidemic” of blindness in premature babies, largely due to the unmonitored use of high levels of oxygen in incubators. Once doctors learned about the connection between oxygen and ROP, careful management of oxygen helped reduce cases. However, as medical care for premature babies improved and even very tiny infants began to survive, ROP unfortunately became a significant issue once again [2].
Who Is Affected?
ROP primarily affects premature infants born very early or with very low birth weights. The earlier a baby is born and the less they weigh at birth, the higher their risk of developing ROP. Babies born before 30-31 weeks of pregnancy or weighing less than 3.3 pounds (1500 grams) are most at risk [3, 4]. While ROP affects infants of all racial and ethnic backgrounds, its incidence can vary globally. In some developing countries, where more premature babies are surviving, ROP is an increasing cause of childhood blindness [4].
Other factors that can increase the risk of ROP include breathing problems, infections, bleeding in the brain, and overall poor health after birth [4].
Diagnosis
ROP is diagnosed through a special eye exam conducted by an ophthalmologist (an eye doctor) who specializes in treating babies. These exams typically start a few weeks after birth for at-risk infants. During the exam, the doctor uses a special light and magnifying tool to examine the retina and check for abnormal blood vessel growth.
ROP is categorized into different “zones” based on the location of the abnormal vessels in the eye and “stages” (from 1 to 5) depending on the severity of the changes [2, 4]. A severe form, sometimes called “plus disease,” indicates that the condition is progressing rapidly [2]. Regular screening exams are crucial for catching ROP early, before it leads to permanent vision loss.
Treatment
Most cases of ROP (stages 1 and 2) are mild and often get better on their own without treatment. However, if ROP progresses to more severe stages (stage 3 and beyond), treatment is necessary to prevent retinal detachment and blindness.
Prognosis
The good news is that with careful screening and timely treatment, many babies with ROP have good vision outcomes. However, even if ROP goes away or is successfully treated, premature babies who had ROP may still have a higher risk for other eye problems later in life, such as:
Regular follow-up eye exams are important throughout childhood and even into adulthood for those who had ROP.
Current Research
Research into ROP is actively ongoing to improve prevention, diagnosis, and treatment. Scientists are exploring:
These research efforts aim to reduce the impact of ROP and ensure the best possible vision for premature babies.
References
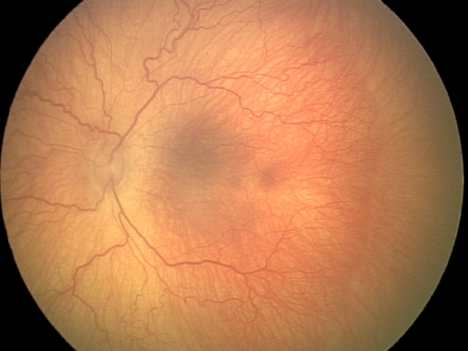
The peripheral retina is not vascularized in this image, with stage 1 ROP (a “demarcation line” positioned between the vascularized and non-vascularized retina) and dilated, tortuous vessels characteristic of “plus disease”.


© 2025 Pediatric Retinal Research Foundation.

